

ADVERTISEMENT
Use of Platelet-rich Plasma in the Treatment of Recalcitrant Sinus Tracts: A Case Series
Index: WOUNDS 2011;23(11):322–327
Abstract: Sinus tract formation is common in a wide variety of wounds and can be difficult to manage. Nonsurgical techniques for treating sinus tracts have generally been disappointing, though many nonsurgical options have been explored including dermal matrix injection, platelet-derived growth factors, fibrin sealant, and phenytoin. This case series explores the treatment of nonhealing chronic wound-related sinus tracts with autologous platelet-rich plasma (PRP) in a series of patients in a single center, hospital-based, chronic wound care center. Methods. PRP was prepared using the Harvest SmartPRep procedure. During processing, the blood was separated into two distinct chambers: one containing packed red blood cells, and the other with autologous platelet concentrate and plasma supernatant. The plasma was injected into the entire sinus tract beginning from the base of the tract. Results. Nine of 12 patients healed, and three did not heal and required other interventions (excision and flap repair). All patients, except one, received only one PRP injection. One case of infection that could be directly attributed to the PRP injection was reported. All other patients experienced no pain, discomfort, or signs or symptoms of infection. Conclusion. PRP injection can be a useful technique in cases of straight, relatively short, persistent sinus tracts.
Introduction
Sinus tract formation is common in a wide variety of wounds.1 Surgical excision of the tract followed by either primary closure or secondary healing is generally considered the treatment of choice. Sinus tract treatment with nonsurgical techniques has been disappointing, though many nonsurgical options have been explored including dermal matrix injection, platelet-derived growth factors, fibrin sealant, and phenytoin.2,3 Fibrin sealant has been used mostly in the perianal region to repair cutaneous sinus tracts, intraoperatively as a hemostatic agent in cardiopulmonary surgery, and as a leakage sealant in colon surgery.4,5 Its use has not been reported for chronic wounds. It is somewhat difficult to apply since it seals quickly, which is not ideal for deep, chronic wound repair. Since it is derived from multiple blood donors, there is a risk of viral and other infectious transmission. Additionally, it is relatively expensive and not reimbursed for wound applications. However, based on the use of fibrin sealant in nonhealing gastrointestinal fistulous and sinus tracts, autologous platelet-rich plasma (PRP) was applied as an alternative, thus combining the known sealant properties of activated fibrin with the added release of growth factors from the platelets and the safety of autologous products. The following case series evaluated the treatment of nonhealing chronic wound-related sinus tracts with autologous PRP in a series of patients in a single center, hospital-based, chronic wound care center.
Fibrin sealant has been used mostly in the perianal region to repair cutaneous sinus tracts, intraoperatively as a hemostatic agent in cardiopulmonary surgery, and as a leakage sealant in colon surgery.4,5 Its use has not been reported for chronic wounds. It is somewhat difficult to apply since it seals quickly, which is not ideal for deep, chronic wound repair. Since it is derived from multiple blood donors, there is a risk of viral and other infectious transmission. Additionally, it is relatively expensive and not reimbursed for wound applications. However, based on the use of fibrin sealant in nonhealing gastrointestinal fistulous and sinus tracts, autologous platelet-rich plasma (PRP) was applied as an alternative, thus combining the known sealant properties of activated fibrin with the added release of growth factors from the platelets and the safety of autologous products. The following case series evaluated the treatment of nonhealing chronic wound-related sinus tracts with autologous PRP in a series of patients in a single center, hospital-based, chronic wound care center. 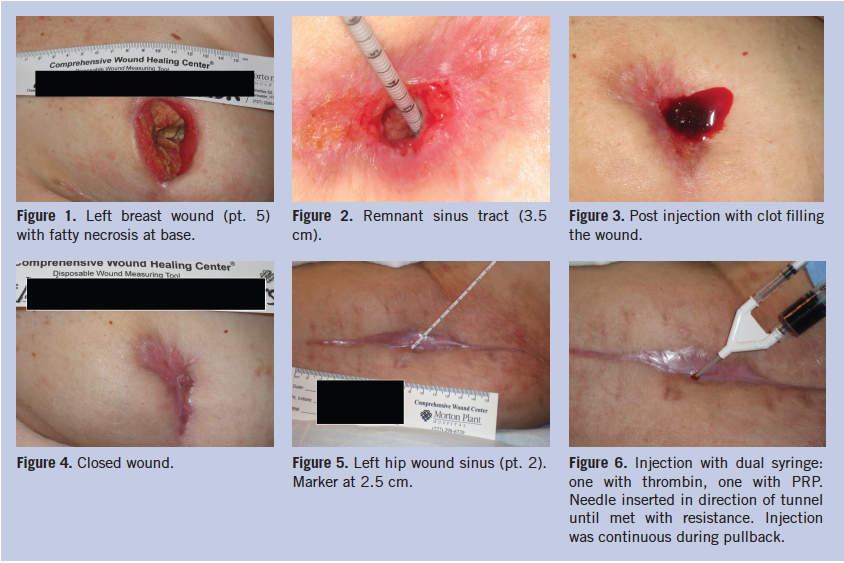
Methods
Patients. All patients were seen in a hospital-based outpatient wound care center and had been receiving various therapies for their wounds and chronic sinus tracts. Wound etiologies, timelines, and products used prior to the PRP are summarized in Table 1. All patients were treated with topical antibiotics/antiseptics (as well as orally if clinical signs/symptoms of infection were present) for 1 to 2 weeks prior to PRP injection, because chronic sinus tracts are frequently associated with bacterial infection or contamination. 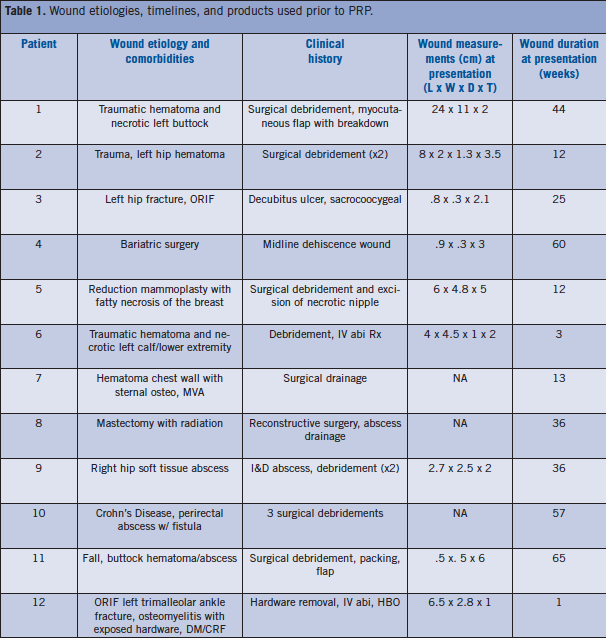 PRP was prepared using the Harvest SmartPRep procedure (Harvest Technologies Corp, Plymouth, MA) by drawing 20 mL of the patient’s venous blood into a syringe with approximately 6 mL of ACD-A (anticoagulant citrate dextrose solution, formula A). Total volume is then transferred to a disposable, dual-chamber blood-processing device. The dual-chamber device is then placed into a centrifuge. During processing, the blood is separated into the two distinct chambers: one containing packed red blood cells, and the other with autologous platelet concentrate and plasma supernatant. The excess plasma is discarded and the platelets are resuspended in the remaining plasma with a volume of approximately 3 cc, which is drawn into a 10 cc syringe. The resultant platelet concentration is in the 800 K/µL–1500 K/µL range. This is then placed as one component of the dual applicator injection catheter, the second component being bovine thrombin in a 1 cc syringe (Figure 6). The applicator tip is then used to inject the entire sinus tract beginning from the base (bottom). After clot formation, which is usually within seconds, a nonadherent primary dressing with secondary gauze bolstering is placed over the wound. The dressing with bolster was left in place undisturbed for 1 week and changed as needed thereafter.
PRP was prepared using the Harvest SmartPRep procedure (Harvest Technologies Corp, Plymouth, MA) by drawing 20 mL of the patient’s venous blood into a syringe with approximately 6 mL of ACD-A (anticoagulant citrate dextrose solution, formula A). Total volume is then transferred to a disposable, dual-chamber blood-processing device. The dual-chamber device is then placed into a centrifuge. During processing, the blood is separated into the two distinct chambers: one containing packed red blood cells, and the other with autologous platelet concentrate and plasma supernatant. The excess plasma is discarded and the platelets are resuspended in the remaining plasma with a volume of approximately 3 cc, which is drawn into a 10 cc syringe. The resultant platelet concentration is in the 800 K/µL–1500 K/µL range. This is then placed as one component of the dual applicator injection catheter, the second component being bovine thrombin in a 1 cc syringe (Figure 6). The applicator tip is then used to inject the entire sinus tract beginning from the base (bottom). After clot formation, which is usually within seconds, a nonadherent primary dressing with secondary gauze bolstering is placed over the wound. The dressing with bolster was left in place undisturbed for 1 week and changed as needed thereafter. 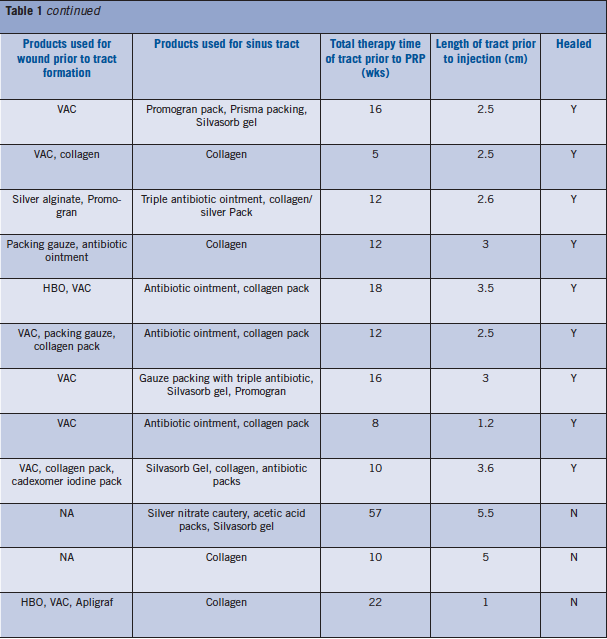
Results
Results are detailed in Table 1. Of the 12 treated patients, nine healed and three did not heal and required other interventions (excision and flap repair). All patients except one (pt. 1) received only one injection of PRP. There was one infection that could be directly attributed to the PRP injection (pt. 10). All other patients experienced no pain, discomfort or signs or symptoms of infection. Of the patients that did not heal, two had the longest tracts with curvature (> 5 cm, pts. 10 and 11) and one had complex comorbidities. Figures 1–4 delineate the progress of pt. 5, and Figures 5 and 6 show the progression of pt. 2.
Discussion
Fibrin sealant has been used in a variety of surgical procedures as a hemostatic agent, as well as a sealant in GI and perirectal fistulas. Its use is limited by cost and the risks associated with multiple donors of human plasma required for processing, since fibrin sealant is made by using multiple cryoprecipitate donors. In addition, it has very quick sealing times, allowing for very little, if any, flow into a deeper wound/tract. 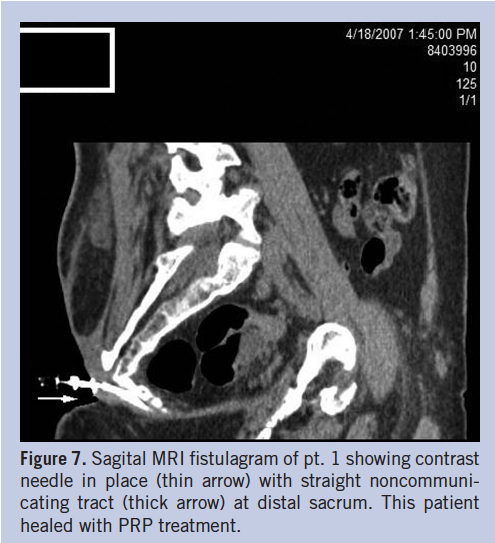 Sinus formation has been documented in a wide variety of wounds and is a difficult problem to treat. The mechanisms of sinus formation involve: infection, liquefaction necrosis, and foreign bodies.1 Based on the knowledge that the platelet clot is essentially composed of fibrin, it was surmised that PRP could have a beneficial effect as a sealant for small, persistent, nonfistulous sinus tracts. PRP has the advantages of being cheaper, readily processed, and autologous, and therefore safe. Additionally, as opposed to fibrin sealant, the degranulation of the platelets and release of various growth factors may enhance healing above and beyond the sealant properties. Many trials have evaluated PRP in chronic open wounds with varying success.6–8 To the authors’ knowledge, this is the first study to trial it specifically for sinus tracts.
Sinus formation has been documented in a wide variety of wounds and is a difficult problem to treat. The mechanisms of sinus formation involve: infection, liquefaction necrosis, and foreign bodies.1 Based on the knowledge that the platelet clot is essentially composed of fibrin, it was surmised that PRP could have a beneficial effect as a sealant for small, persistent, nonfistulous sinus tracts. PRP has the advantages of being cheaper, readily processed, and autologous, and therefore safe. Additionally, as opposed to fibrin sealant, the degranulation of the platelets and release of various growth factors may enhance healing above and beyond the sealant properties. Many trials have evaluated PRP in chronic open wounds with varying success.6–8 To the authors’ knowledge, this is the first study to trial it specifically for sinus tracts.  The use of PRP in wound healing has focused on two basic forms: platelet lysate, and platelet releasate, a form of which is called platelet gel. Platelet lysate, as the name implies, is obtained by collection of the platelet supernatant followed by freezing to result in lysis and degranulation of the platelets without the addition of platelet activators. The resultant frozen product is then thawed and applied to the wound bed with gauze or collagen granules. Platelet releasate involves the same general technique for centrifuging and obtaining the cell-poor platelet concentrate, but this is then activated with thrombin (usually bovine) to induce release of the platelet alpha granules. The resultant gel-like material is applied directly to the wound. PRP in the form of releasate is most commonly used today and is the form that was used in this series.
The use of PRP in wound healing has focused on two basic forms: platelet lysate, and platelet releasate, a form of which is called platelet gel. Platelet lysate, as the name implies, is obtained by collection of the platelet supernatant followed by freezing to result in lysis and degranulation of the platelets without the addition of platelet activators. The resultant frozen product is then thawed and applied to the wound bed with gauze or collagen granules. Platelet releasate involves the same general technique for centrifuging and obtaining the cell-poor platelet concentrate, but this is then activated with thrombin (usually bovine) to induce release of the platelet alpha granules. The resultant gel-like material is applied directly to the wound. PRP in the form of releasate is most commonly used today and is the form that was used in this series.
Conclusion
PRP can be a useful alternative in nonhealing sinus tracts. The most important aspect in this series of patients was to ensure proper bacterial control within the sinus tract in order to avoid the development of infection. Thus tracts were treated prior to injection with appropriate antiseptic/antibiotic packing for 1 to 2 weeks. The authors recommend only injecting tracts that are relatively straight, as any curvature in the course of the tract could induce dead space formation and subsequent abscess development. There was a low threshold for imaging via sinogram to avoid injecting long tracts, curved tracts, tracts with significant out-pouching, complex tracts, and tracts with extension into visceral organs, hardware, or infected bone (Figure 7). Of the three patients whose wounds did not heal, two (pt. 10 and pt. 11) had long (> 5 cm) tracts with curved courses and complex anatomy; one (pt. 12) had complex comorbidities and chronic renal failure. All straight tracts with < 5 cm length healed. Injection should start at the base of the wound to fill the entire tract with continuous injection during pullback. PRP injection can be a useful technique in cases of straight, relatively short, persistent sinus tracts.
References
1. Butcher M. Management of wound sinuses. J Wound Care. 1999;8(9):451–454. 2. Anstead GM, Hart LM, Sunahara JF, Liter ME. Phenytoin in wound healing. Ann Pharmacother. 1996;30(7-8):768–775. 3. Banta MN, Eaglstein WH, Kirsner RS. Healing of refractory sinus tracts by dermal matrix injection with Cymetra. Dermatol Surg. 2003;29(8):863–866. 4. Park JJ, Cintron JR, Orsay CP, et al. Repair of chronic anorectal fistulae using commercial fibrin sealant. Arch Surg. 2000;135(2):166–169. 5. Mintz PD, Mayers L, Avery N, Flanagan HL, Burks SG, Spotnitz WD. Fibrin sealant: clinical use and the development of the University of Virginia Tissue Adhesive Center. Ann Clin Lab Sci. 2001;31(1):108–118. 6. Knighton DR, Fiegle VD, Doucette MM, Fylling CP, Cerra FB. The use of topically applied platelet growth factors in chronic nonhealing wounds: a review. WOUNDS. 1989;1(1):77–78. 7. Holloway GA, Steed DL, DeMarco MJ, et al. A randomized, controlled dose response trial of activated platelet supernatant, topical CT-102 in chronic, nonhealing, diabetic wounds. WOUNDS. 1993;5(4):160–168. 8. Driver VR, Hanft J, Fylling CP, Beriou JM; Autologel Diabetic Foot Ulcer Study Group. A prospective, randomized, controlled trial of autologous platelet-rich plasma gel for the treatment of diabetic foot ulcers. Ostomy Wound Manage. 2006;52(6):68–74. The authors are from the Morton Plant Hospital Wound Care Center, Clearwater, FL. Address correspondence to: Reynald C. Allam, MD, MBA 455 Pinellas St., Ste 300 Clearwater, FL 33756 727-462-7000 rallam1@hotmail.com







